The Way We Live Now: AIDS, 25 Years Later
Last week marked the 25th anniversary of the first reported AIDS cases. Survivors, recalling the days before AIDS had a name, often invoke an experience akin to walking unguided in the dark. Because it was first detected in urban gay populations—most notably in San Francisco and New York City—AIDS was identified as a "gay cancer." Nobody had answers to the questions surrounding the deaths of so many young gay men. Ostracism reigned, and policy makers at the highest levels of power retreated into denial and dismissal of an epidemic that today stretches around the globe.
The AIDS crisis polarized the gay community, but it was also the catalyst for previously unknown levels of activism among a very vocal segment of the gay population. Gay Men's Health Crisis and Act Up, among other groups, propelled the topic of health care equality for gays onto a national stage. No other health care crisis in modern history benefited from such an organized response and from so small a disenfranchised group. It took an invasive and initially life-claiming illness to position gay rights front and center in the American consciousness.
For many of us, too young to have been sexually active and aware of the emerging health crisis, it's difficult to fathom the uncertainty and fear that swirled around the disease early on. And we can't begin to understand the obstacles faced by early AIDS warriors. As the memories of those early days, and our early defenders, fade and pass on, the legacy of loss and sorrow dims ever so incrementally. Yet the debt we owe these men and women is far greater than we could ever repay.
In the early 1980s I was a high school junior navigating the traps of adolescence. While my sexual preference for men had already revealed itself, I hid behind a creaky facade of heterosexuality. News of a murderous "cancer" among gay men was far from my consciousness, though I'm certain the Time magazine cover stories and nightly news coverage echoed nearby.
Today I look around in wonder at the trajectory of the disease. Whenever I can, I try to coax stories of the "early" days from my friends who lived them. These people are old enough to have observed the evolution of AIDS from anonymous killer to high profile cause célèbre and finally to its current status as a grinding global health crisis. And as Dr. Abigail Zuger's article from a recent edition of the New York Times reminds us, our response to the disease has changed too. AIDS may still be an elusive phantom, but it's not the enigma it once was. Determined scientists have chipped its mystery away.
 The pathos surrounding its claim on so many lives has inspired some of the most moving literature of the late 20th century. Tony Kushner's monumental play Angels in America showed us that AIDS didn't discriminate as it ticked off people across the socioeconomic spectrum. This great play also revealed the hypocrisy of the era, an attitude towards the ailing that only made their suffering worse. Kushner's hopefulness couldn't be dampened, however.
The pathos surrounding its claim on so many lives has inspired some of the most moving literature of the late 20th century. Tony Kushner's monumental play Angels in America showed us that AIDS didn't discriminate as it ticked off people across the socioeconomic spectrum. This great play also revealed the hypocrisy of the era, an attitude towards the ailing that only made their suffering worse. Kushner's hopefulness couldn't be dampened, however.  In his great work one of the most surprising attitudinal turnarounds comes in the guise of one of the main characters, a mother (played by Meryl Streep in the HBO production of Kushner's screenplay based on his stage play) who migrates from Salt Lake City to the boroughs of New York City in hopes of putting back together the shards of her gay son's broken marriage. This brittle Mormon lady, so obviously out of her element in the chaos of New York's gay culture, demonstrates a steely grace towards the play's protagonist, Prior Walter, a "stereotypical" gay man. When he opens his shirt revealing a Kaposi's sarcoma lesion, her eyes caress his skin, she looks at him squarely and says, "It's just a cancer. Nothing more. Nothing more human than that." Kushner knocks the legs out from under the oppressive stigma of AIDS and levels the playing field. Nothing more human than that, indeed.
In his great work one of the most surprising attitudinal turnarounds comes in the guise of one of the main characters, a mother (played by Meryl Streep in the HBO production of Kushner's screenplay based on his stage play) who migrates from Salt Lake City to the boroughs of New York City in hopes of putting back together the shards of her gay son's broken marriage. This brittle Mormon lady, so obviously out of her element in the chaos of New York's gay culture, demonstrates a steely grace towards the play's protagonist, Prior Walter, a "stereotypical" gay man. When he opens his shirt revealing a Kaposi's sarcoma lesion, her eyes caress his skin, she looks at him squarely and says, "It's just a cancer. Nothing more. Nothing more human than that." Kushner knocks the legs out from under the oppressive stigma of AIDS and levels the playing field. Nothing more human than that, indeed. Larry Kramer's The Normal Heart tells the story of the beginnings of an organized response to the disease by a privileged group of gay Manhattanites. It's an autobiographical rendering of the emergence of hope for dying men in the form of Gay Men's Health Crisis. But it's also a portrait of loss as the play's main character Ned Weeks watches his young lover's body, and mind, deteriorate and slip away.
Larry Kramer's The Normal Heart tells the story of the beginnings of an organized response to the disease by a privileged group of gay Manhattanites. It's an autobiographical rendering of the emergence of hope for dying men in the form of Gay Men's Health Crisis. But it's also a portrait of loss as the play's main character Ned Weeks watches his young lover's body, and mind, deteriorate and slip away.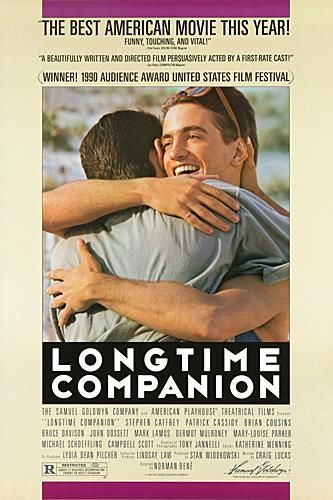 In the film Longtime Companion writer Craig Lucas explored the changing dynamics of a group of friends who watch as members of their close-knit circle succumb to AIDS. Through this well-connected cadre of gay men, the film traces the chronology of the AIDS epidemic. Although the film was criticized for focusing strictly on the reach of AIDS into the lives of middle and upper-middle class white men, it was one of the first cinematic glimpses into the way the disease transformed our lives.
In the film Longtime Companion writer Craig Lucas explored the changing dynamics of a group of friends who watch as members of their close-knit circle succumb to AIDS. Through this well-connected cadre of gay men, the film traces the chronology of the AIDS epidemic. Although the film was criticized for focusing strictly on the reach of AIDS into the lives of middle and upper-middle class white men, it was one of the first cinematic glimpses into the way the disease transformed our lives.The movie begins on the shores of Fire Island's Pines community to the strains of Deborah Harry's The Tide Is High. These are the waning days of innocent revelry for gay men at this iconic resort. By the end of the movie, some ten years later, most of the characters from the earlier scenes are dead. We are back on the same stretch of beach with three of the remaining friends who wonder what effect a cure for the disease might have on gays. "It would be like the end of World War II," one character, played by Mary Louise Parker, remarks. It's a delicate and poignant scene of despair and sadness.
 Hundreds of books, articles, reports, and essays by writers including Edmund White, Andrew Holleran, Susan Sontag, Larry Kramer, Randy Shilts, Paul Monette, and Reynolds Price have described the multi-layered meaning of life in the time of AIDS. An equal number of films on the subject have guided us through the emotions of fear, frustration, anger, despondency, and crushing loss.
Hundreds of books, articles, reports, and essays by writers including Edmund White, Andrew Holleran, Susan Sontag, Larry Kramer, Randy Shilts, Paul Monette, and Reynolds Price have described the multi-layered meaning of life in the time of AIDS. An equal number of films on the subject have guided us through the emotions of fear, frustration, anger, despondency, and crushing loss.The specter of AIDS has long since moved beyond gays. And, in fact, the demographics were always far wider than we allowed our imaginations to travel. Gays were only its first public face. Hemophiliacs, and any other person needing blood transfusions, too were especially vulnerable in the early years before blood tests to detect the virus were developed. Today, there is debate about whether the numbers of seroconversions to HIV-positive status are rising. Almost everybody involved in studying the shifting demographics of the virus, however, agrees that urban African-American males are counted increasingly among the numbers of new infections. All eyes, and intervention efforts, are focused on the African continent as the disease continues to multiply among the peoples of all nations there.
Abigail Zuger writes about the state of affairs today, twenty-five years after the first cases of AIDS were reported. In 2001, twenty years past the glimmers of AIDS devastation, Jennifer Steinhauer wrote about some of the long-lasting cultural changes brought about by the disease. Each article, separated by five years, is both compelling and chilling. It's difficult to imagine a time before this record of human devastation.
We talk about AIDS. We remember friends who have died from its complicating factors. We struggle to comprehend its reach. We wonder about a cure. We scratch our heads at the risks some us still take with all the knowledge at our fingertips on how one incautious involvement can alter our lives forever. We try to understand the contradictory nature of the human mind. And we marvel at how humanity continues to press on in the face of such despair and incalculable loss. And, then we talk about AIDS some more—to keep consciousness and awareness present, to rattle our hearts and minds to action.
AIDS, at 25, Offers No Easy Answers
By ABIGAIL ZUGER, M.D.
Instinctively, the first thing we want to know about a disease is whether it is going to kill us. As the Talmud says, pretty much all the rest is commentary. Twenty-five years ago, this was the only question about AIDS we could answer with any certainty; how disorienting it is that now, vast quantities of commentary later, it is the only question we really cannot answer well at all.
By now, those of us in the AIDS business long term have cared for thousands of patients. No one with that kind of personal experience can doubt for a moment the malignant potential of H.I.V. or the lifesaving capabilities of the drugs developed against it. But there are also now hundreds of footnotes and exceptions and modifications to those two facts that make the big picture ever murkier.
Not everyone who is infected gets sick. Not everyone who is treated gets well. Some people progress along the road from initial infection to progressive immune deficiency to life-threatening illness at the expected pace, then with treatment head right back again to health. Others stall along the way, sick or well, defying our dire predictions and happy reassurances alike.
Patients newly diagnosed throng into our clinics, many of them very young, and utterly underwhelmed by their infection. They know for a fact that the new drugs will make everything all right. I gave one of them his diagnosis on a hospital ward last year. "Try not to worry too much," I told him as he stared blankly at his computer screen; it turned out he was more concerned by his weak wireless connection than his new status as a person with advanced AIDS.
He was scrawny, spotted purple, with AIDS-related cancer all over his mouth and lungs, a flash from the grim past. We gave him all the magic drugs; he died five months later, age 23.
But for every memento mori like him, there are hundreds we save. As death rates fall, the numbers living with infection rise. As hospitals empty, the outpatient clinics overflow. The more drugs we have, the more drugs we need to mop up behind them, treating side effects and failures. All in all, we have an expensive little wellness industry on our hands, often with budgets so badly out of date we can barely keep up with it all.
Our clinic waiting rooms have always been strange places, the sick and the healthy all bundled in there together, the gaunt and the robust side by side.
But even there, things are getting stranger. That skeletal fellow reading a magazine, skin pulled taut over his skull, folds of denim covering his wasted legs, is actually one of our big successes. He is perfectly well, at least as far as his H.I.V. infection goes. Ten years ago he was dying of AIDS; now he is living with it — or, more accurately, living almost without it, his immune system normal, no trace of virus detectable in his blood. It is the lifesaving drugs that have transformed his appearance like this, leaching the fat from his body even as they clear the virus from his blood.
He is another memento mori, for it is impossible to look at him and not see fatal illness, and yet as far as we know he will live a full life, untroubled by AIDS. Except, of course, that he now has other problems. The drugs have knocked his metabolism all out of whack: his body may be skeletal but his bloodstream is full of sugar and fat damaging his heart, liver and kidneys.
His appearance makes it hard for him to find work; the plastic surgery to fix his face a few years ago led to only temporary improvement, and he cannot afford more. Still, he continues to take the culprit medications precisely, day after day.
The vigorous man next to him, muscles bulging out of his shirt, is also in disguise. Ten years ago he was dying of AIDS, and now we think he still is, although we cannot be absolutely sure. His blood tests are terrible: his immune system in a shambles, the virus in his blood resistant to all the drugs we have.
Yet, for reasons no one can explain, he continues to thrive on these drugs, with no side effects. He too has had plastic surgery, for, he tells us, he plans to "live life to the fullest," by exercising, partying and staying as beautiful as possible for as long as possible. It is anyone's guess if his party has weeks, years or decades yet to run.
To look at him, dance with him, date him, you'd never know anything was wrong. But anyone who catches his virus may be in for a bad time; he must be careful, we tell him over and over and over again.
And between those two extremes we have patients scattered at every possible point: men and women who cruise on their medications with no problems at all, and those who never stabilize on them and die of AIDS; those who never take them properly and slowly deteriorate and those who never take them properly and still do fine; those who refuse them until it is too late, and those who never need them at all; those who leave AIDS far behind only to die from lung cancer or breast cancer or liver failure, and those few who are killed by the medications themselves.
And so, when we welcome a new patient into our world, one whose fated place on this grid is still unclear, and that patient asks us, as most do, whether this illness is going to kill him or not, it often takes a bit of mental stammering before we hazard an answer.
Twenty-five years ago, treading water in that black sea of untreatable illness, we had only one answer to give. Only a lunatic would look back to those days with nostalgia, but certain parts of them have, inevitably, taken on that glow tricks of memory can sometimes confer on the terrible past. With no possibility of saving our patients, life was sadder but far simpler. The big war was already lost, so we could concentrate on small victories instead.
Now, a complete rundown of all the news from the front would take hours. Risk of death from AIDS: way down. Risk of death from other things: going up. Risk of drug reaction: depends. Risk of fatal drug reaction: low but not zero. Risk of drug resistance: gets higher every year. The statistics change almost hourly as new treatments appear. It is all too cold, too mathematical, too scary to dump on the head of a sick, frightened person. So we simplify. "We have good treatments now," we say. "You should do fine."
The bottom line is clear enough: once, not so long ago, we were working in another universe. Now we have simply rejoined the carnival of modern medicine, noisy and exhilarating, confusing and contradictory, fueled by the eternal balancing of benefits and risks.
You can win big, and why shouldn't you, with the usual fail-safe combination of luck and money (and lots of it). You have our very best hopes, so step right up: we peddle big miracles but, alas, offer no guarantees.
JUN 04, 2001
AIDS Altered the Fabric of New York in Ways Subtle and Vast
By JENNIFER STEINHAUER
Before AIDS, there was no breast cancer walk in Central Park. Babies needing foster parents languished in hospitals for weeks, sometimes years. Clinics doled out medicines and sent the sick on their way, rarely looking at what it was in their lives that helped to make them ill.
In many ways, New York City after AIDS is somewhat like America after World War II — a place physically unscathed yet socially transformed, missing slices of entire generations of its citizens, its lasting effects at times concrete and at others evanescent.
It changed the speed at which social services moved, and changed the people with whom city politicians curried favor. It made patients with all types of critical illnesses press their doctors harder for information, and took public health workers out of their offices and into neighborhoods where they learned why certain diseases were prevalent.
AIDS morphed the insurance, fashion, philanthropic, health care, real estate and music industries, and altered the hip quotient among the social set's choices in entertainment and charitable causes.
Many of these changes, particularly those involving health care, were boosted along by myriad other factors — managed care, a booming economy and the Internet, to name just a few.
But there is no question that AIDS — which has killed 75,000 New Yorkers, nearly 20 percent of the Americans who have died of AIDS since it was first identified 20 years ago — altered the city in ways both so widespread and at times so subtle that those shifts are no longer consciously associated with the disease. And while the rest of the country was also reeling from the epidemic, many lasting cultural changes began here.
"AIDS reached into almost every segment of New York and society in different ways," said Carol Levine, a former director of the Citizens Commission on AIDS. "It was horribly painful, and it was intriguing. It could not be contained into one thing. It was a disease, it was a social problem and it did not fit into a neat little conceptual framework to solve. It has been instructive to all of us. But at a horrible cost."
New York, the birthplace of the Gay Men's Health Crisis and Act Up, was among the first American cities where groups concerned with other diseases learned from AIDS groups how to successfully hector the government for access to new treatments and services.
"I think there is a very direct relationship between breast cancer activism and AIDS activists," said Ann Northrop, a longtime Act Up member. "Act Up created the concept of patient empowerment, it specifically ruled out that phrase `victim,' and that was a whole new concept. Suddenly there was patient involvement in issues like drug approval."
The AIDS walk begot breast cancer walks, and public parades for other illnesses are now as much a rite of spring in Central Park as softball and Shakespeare. And while few groups staged the "die-ins" favored by Act Up that tied up Holland Tunnel traffic and turned Grand Central into a macabre rush-hour graveyard of the living, many emulated the strategy.
"Liver and breast cancer groups would come and watch us," remembered Larry Kramer, Act Up's founder. Susan Safire, the executive director for Share, a breast and ovarian cancer support group in New York, agreed that while radical activism was not her group's taste, her group was quiet before AIDS. "There is absolutely more patient empowerment now," Ms. Safire said. "I say `thank you' to AIDS activists, because they led the way."
For gays who did not take part in the coming out in the 1960's, AIDS brought about an inevitable if unwelcome second opportunity. Some men who became visibly ill, for instance, were suddenly out to their co-workers. Others whose past political acts were limited to voting suddenly found themselves taking to the streets.
"What AIDS did was to bring many more people out of the closet and politicize the group of privileged white men who thought they had already entered the mainstream," said Martin Duberman, a pre-eminent gay historian. "Then obviously the movement swelled."
Gays have become a political constituency in the city, one that rivals traditional voting blocs like religious Jews and African- Americans in some neighborhoods.
"The gay community was important in the 1989 mayoralty," said Mark Green, the public advocate who is running for mayor. "But it is geometrically more important now. On the Democratic side, there are several important gay leaders that candidates predictably meet with, talk with and woo." Mr. Green, apparently taking no chances, recently joined the influential Gay and Lesbian Independent Democrats.
Before 1991, there was not an openly gay member of the City Council. But that year, Thomas K. Duane and Liz J. Abzug, the two gay candidates, fought over the Third District, where Mr. Duane, who revealed during that campaign that he was H.I.V.-positive, ultimately prevailed, and now there are several gay elected officials in New York, a shift in political representation that has fanned out around the country.
"On a practical level," said Ronald G. Bayer, a professor of public health at Columbia University, "the gay community has emerged as a political constituency that has to be dealt with. It is legitimization through disaster."
Dealing With Disease
In the mid-1980's, an unprecedented move in the State Health Department changed the way hospitals in New York cared for those with AIDS, with sizable implications for hospitals dealing with future illnesses.
In 1983, the Health Department set up the AIDS Institute to focus attention on and distribute money for the epidemic. At that time, hospitals and medical clinics were loath to care for AIDS patients, because of their costly and complicated needs, and out of fear over the stigma they would attract to the institutions.
With a clever Medicaid trick, the institute solved its problem. It offered hospitals the chance to be named AIDS Designated Care Centers, in exchange for Medicaid payments that were 20 percent higher than normal rates for Medicaid patients. New York hospitals leapt at the chance to become so designated.
What hospitals had to do was come up with a plan giving AIDS patients a sort of buffet of services, rather than just minimal health care to keep them alive. "It was not just going to be an infectious-disease person who was provider of care," said Dennis Whalen, a deputy health commissioner. "AIDS and H.I.V. patients required an interdisciplinary team of doctors, nutritionists, social workers, psychiatric workers, all to be put together in team approach." This special Medicaid rate system was later replicated for tuberculosis in the late 1980's.
And the system of coordinated care that the hospitals devised for AIDS has trickled down into the management of other illnesses, like asthma, strokes and cancer. To have a cancer patient wander an entire hospital campus for chemotherapy, radiation and psychotherapy is almost anathema in many hospitals; before AIDS it was standard.
In some ways, the legacy of coordinated care can even be seen in how the Health Department has attacked the West Nile virus. Health care workers talked to wildlife experts who in turn talked to scientists studying infectious diseases.
While many people with AIDS ended up on Medicaid, the collapse of one corner of the insurance market and the rapid rise of the uninsured in New York can also be traced in large part to the disease.
"One thing the epidemic did was kill the direct-pay individual insurance market in New York," said Bruce C. Vladeck, director of the Institute for Medicare Practices at the Mount Sinai School of Medicine. He estimated that roughly 550,000 New Yorkers who were unemployed or self-employed bought individual health plans before AIDS. But AIDS brought too many sick people into that market, which responded by raising the rates to the sky.
"This contributed to the financial crisis of Blue Cross and eventually caused the price of that coverage to rise substantially," Mr. Vladeck said. The number of New Yorkers in individual plans has fallen to about 72,000, according to the State Department of Insurance, and many people — no longer just those with AIDS — who cannot afford insurance simply go without. There are now roughly 3.1 million uninsured New Yorkers.
Taking its cues from grass-roots groups like the Gay Men's Health Crisis, the Health Department began to reach out directly to people living in specific communities where problems ranging from infant mortality to asthma seem the most stubborn, rather than just working through local clinics.
"Probably 20 years ago we would have not picked up on the opportunity to engage communities in their own self-advocacy," said Dr. Neal L. Cohen, the city's health commissioner.
In one case, health care workers descended on a neighborhood to discuss methods for quitting smoking; it was learned that what the residents, many of them elderly, really cared about was the fact that people kept falling on the broken sidewalks.
How the Fun Changed
The seeds of cool are almost always planted among some marginalized group, and in the 1970's, gay men led the way in fashion and music, from Studio 54 and its predecessors, to the Pines on Fire Island, where Yves St. Laurent saw revelers in painter pants and jelly shoes and appropriated the look for his collection.
"Gays used to be the people that the record industry tested records on," said Hal Rubenstein, an editor at InStyle magazine. "They would take pressings from the studio to Paradise Garage or the Sandpiper in Fire Island and preview them out there. Lots of people took their cultural cues from gay people, because they were the taste makers and we were having more fun than everyone else."
The collapse of the Fire Island scene — 25 percent of the homes there went unrented during the summers of the mid-1980's — and of disco made way for a new urban music movement, hip-hop. A booming economy helped fuel a change in entertainment venues and trendy lifestyles that focused more on money and glamour than on outsider hipness, many popular culture experts say.
And cultural icons began to reappear from more traditional corridors, like Hollywood, with its stars and their stylists.
"Things that are safe are seen as much more desirable now,' said the writer Bob Colacello, a former editor of Interview magazine. "Risk is limited to Wall Street, and the wild life is at the White House and Gracie Mansion."
Charities became hot: dance parties for the homebound meal service God's Love We Deliver, the Design Industries Foundation Fighting AIDS annual holiday gala, fund- raisers at Barneys attended by Madonna. "AIDS made fund-raising hip," said Simon Doonan, the creative director of Barneys New York. "Before that, charities were the purview of Park Avenue ladies."
And the talent pool in fashion shifted in an unexpected direction. "AIDS did open up the industry to women," said Stan Herman, president of the Council of Fashion Designers of America. In the late 1980's, many fashion companies shied away from hiring men, fearing they would die and not wanting to insure them, he said.
New Urgency and Shift in Focus
AIDS brought an immediacy to social services that simply did not exist before, but whose legacy lingers. Intractable problems like poverty, addiction and homelessness were given a new urgency because many of those who suffered from them were now also dying, and quickly.
For example, before AIDS, drug policies in New York City focused almost entirely on getting people off drugs. Groups that provided housing for poor people recovering from their addictions often required users to be drug-free for several months. "AIDS upped the ante," said the Rev. Lisa Hill, director of special projects at the West Side Federation for Senior and Supportive Housing Inc., which runs apartment buildings for the elderly and those with AIDS.
But unlike past drug users, whose treatment and relapse trajectory tended to snake over the course of many years, addicts with AIDS were dying and needed housing quickly. Rules had to change. Instead of saying people could not use drugs, house rules at group homes were altered to reflect that people now should not steal, or destroy property, Ms. Hill said.
Soon, the shift in focus from abstinence to what is known as harm reduction was in place for all addicts. "You see someone who is using and homeless and doesn't have AIDS," she said. "We can't say" that they deserve services any less quickly, she said.
"Harm reduction is an amorphous movement that says, `Not everyone is going to stop using, so what are the ways that you are going to decrease harm?' " Ms. Hill said. "If AIDS is transmitted through drug use, how about switching to snorting? Or clean needles?"
The world of social services for children was also altered.
For one thing, the availability and quality of foster care improved along with increased need, said Gretchen Buchenholz, executive director of the Association to Benefit Children, a nonprofit agency that brought two lawsuits intended to fast track "boarder babies," those children born H.I.V.-positive or with crack in their systems, who were left behind in hospitals, into foster care.
The growing need led nonprofit agencies to lobby the government for more money to recruit appropriate foster parents. The effort moved into neighborhoods, with social service workers approaching potential parents directly or working though places like churches. In 1985, 16,618 children were placed in foster homes; in 1991, the number rose to 49,163. (It is now at 31,689.)
"AIDS and H.I.V. helped the policy makers and administrators understand the importance of recruiting people who had informed consent" about the difficulties and the realities of the children they were taking in, said Eric Brettschneider, who ran the city's child welfare agency in the Koch administration.
And in many ways, many people in social services felt compelled to simply speed up the way they worked.
"We learned the measuring of what is important," Ms. Hill said. "With mental illness, for instance, getting better is not necessarily stopping having mental illness. There are other kinds of getting better, but it comes down to how you measure better now. Is it a job having a $50,000, or is it being able to have relationships with other people or not being hospitalized? There is more focus now on living in the moment in our work now. AIDS let us never forget that."
Tenant and Family Law Reshaped
In 1989, the State Court of Appeals overturned rulings that blocked a man from living in a rent-controlled Manhattan apartment that he had shared with a man who died of AIDS. That ruling led to numerous challenges to the state rent-control laws and to co-op boards. "Braschi is not limited to gay couples," said Nan D. Hunter, a professor of law at Brooklyn Law School, referring to the name of the plaintiff in that case. "That whole constellation affects unmarried heterosexuals with committed relationships, lesbian couples and other kinds of extended families which don't include a husband and wife in the area of landlord tenant law." The case reconstituted the idea of family in New York; in 1992, the city began allowing unmarried couples that have registered with the city clerk's office as domestic partners, an outgrowth of these early AIDS cases, say many.
And in 1986, School Board 27 in Queens tried unsuccessfully to sue the Board of Education for permitting an 8-year-old with AIDS to stay in the classroom, setting the stage for other cases of students with communicable diseases.
"Public health law was really a pretty dormant area until AIDS happened," Ms. Hunter said. "The state passed a statute protecting the privacy of AIDS medical records, which brought us to the whole issue of privacy of medical records generally."
A Legacy of Pain and Loss
The funerals have lessened. Drugs have elongated lives and greatly reduced H.I.V. transmissions to infants. Social services are more plentiful. But the lasting wound festers in disparate corners of New York. The scar of AIDS, said Dr. Bayer of Columbia University, is "that which is not here."
Ms. Buchenholz is surprised that the memories still bring choking tears.
"We watched families bury their babies," she said. "We watched Alfredo bury his wife, then his little boy. We watched Laurie die in her teacher's arms. So many of those children died in our arms. You watched kids start to walk and then start to run, and then you watched yourself lose them. It was the hardest time."
Mr. Doonan, of Barneys, cannot even count all the friends he has lost. "I have a whole new set of friends, and they are all younger," he said. "What do you say when you were a group of six and four of them have died? I don't go near them anymore. In order to continue your life you have to build bridges with new groups of people who don't have that experience.
"I think there are enormous holes left by the people who passed away," he added. "I don't think I have experienced any joy from surviving it. I just think what a nightmare it all was."
posted by Michael Joseph Owens at 3:29 PM
![]()
![]()